
The Proxy Paradox
Medical school admissions may be getting more proxy-driven at exactly the moment everyone says they are getting more holistic.

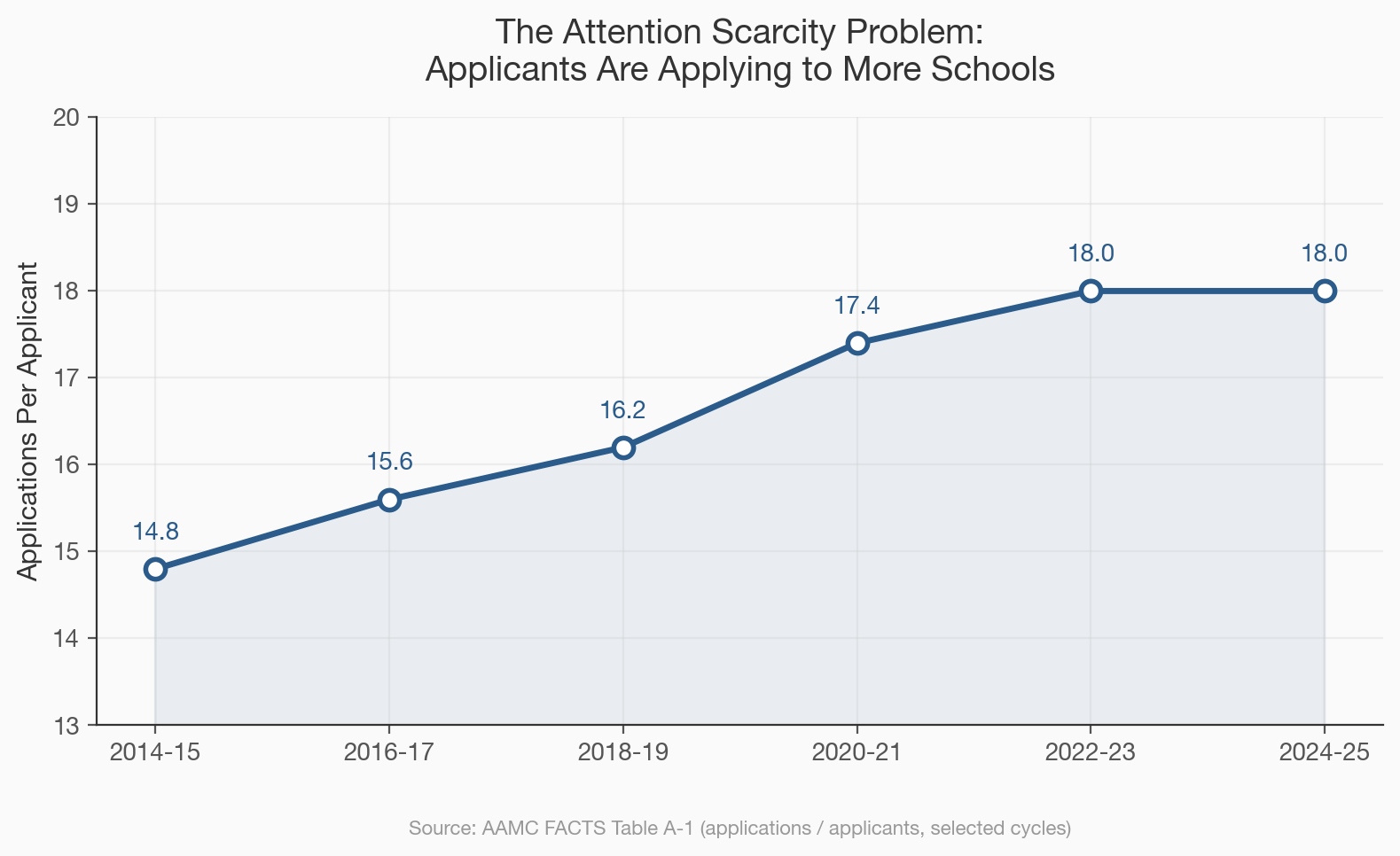
In the 2025 application cycle, 54,699 people applied to medical school in the United States, each submitting an average of 18 applications through AMCAS, a figure that has climbed steadily from the mid-teens over the past decade, which means that the total volume of application material landing on admissions desks has grown faster than the applicant pool itself, and the people reading those applications, the committee members who describe their process as “holistic review,” now face a mathematical problem that no amount of mission-statement language can solve: there are too many polished, qualified, carefully packaged applicants for the number of humans available to evaluate them, and when the reading load outpaces the reading capacity, committees do not become more thoughtful, they reach for shortcuts.
The word admissions committees use for this process is holistic, a term the AAMC has promoted for over a decade to describe an approach that considers the whole applicant rather than reducing candidacy to
a GPA and an MCAT score, and on paper the shift sounds like progress, because the old system was transparently numeric, a sorting algorithm that filtered applicants by standardized metrics before anyone bothered to read their personal statement, while the new system promises to weigh experiences, identity, mission alignment, and the ineffable quality of being a person who will make a good doctor. But two structural changes have quietly undermined the holistic premise at the exact moment it was supposed to be ascendant, and the result is a system that may be more proxy-dependent than the one it replaced, even as it speaks the language of nuance.
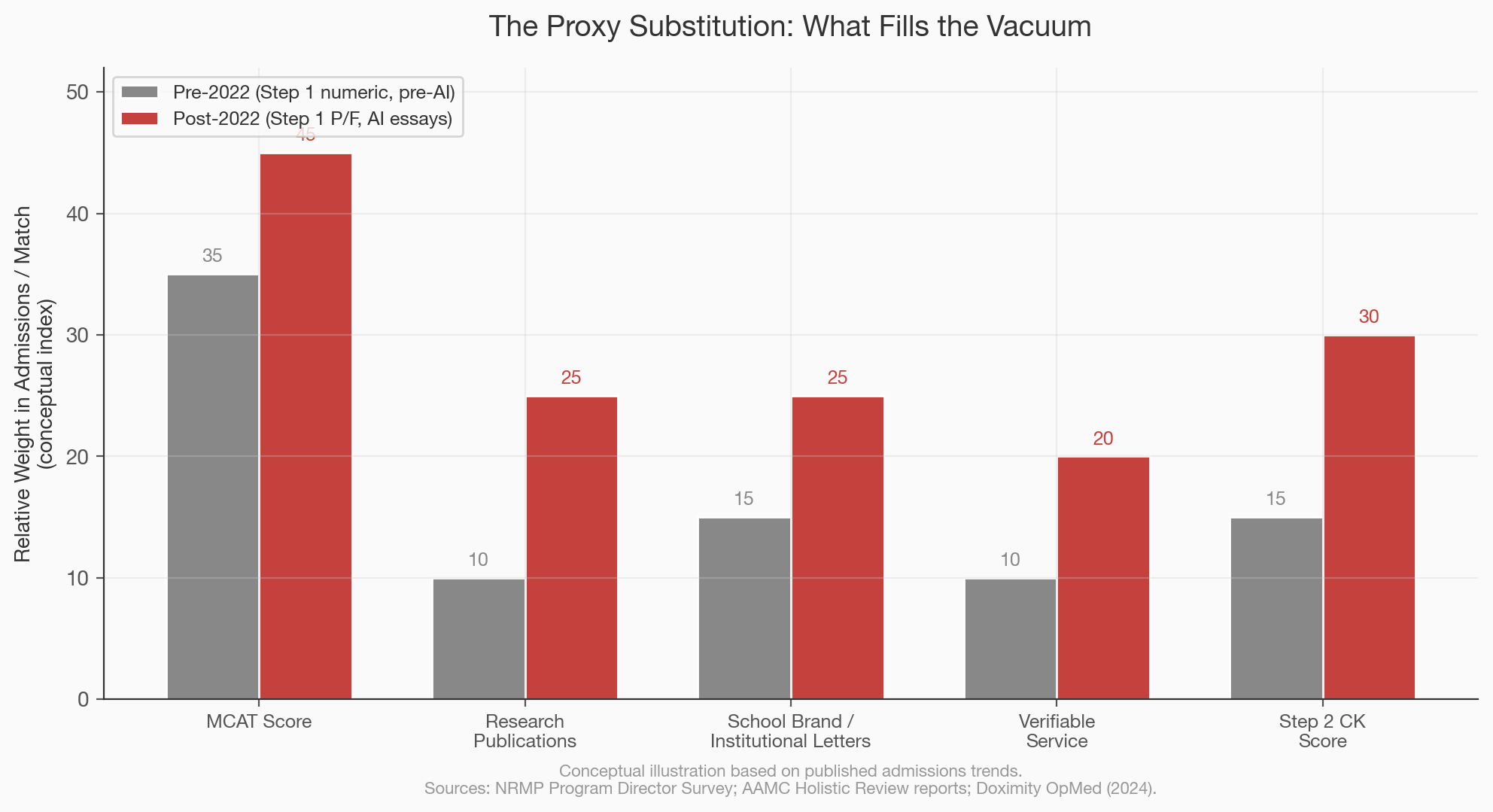
The first structural change came from downstream. In January 2022, USMLE Step 1, the board exam that medical students take after their second year, switched from a three-digit numeric score to pass/fail reporting, eliminating one of the most powerful sorting mechanisms in the residency match, the process by which medical school graduates are assigned to training programs. Step 1 scores had functioned for decades as a blunt but legible signal: a 250 told a program director something different than a 220, and competitive specialties like dermatology and orthopedic surgery used the score as a first-pass filter. When that number disappeared, program directors did not stop filtering, they substituted, shifting weight to Step 2 CK scores (which remain numeric), to research publication counts, to the prestige of the applicant’s medical school, and to institutional letters of recommendation whose credibility depends almost entirely on the reputation of the person signing them. A Doximity analysis found that the transition created what one author called a “new arms race” in research and extracurriculars, as students scrambled to replace the lost signal with other legible credentials, and residency programs, now unable to sort by Step 1, leaned harder on proxies that correlate with institutional access rather than clinical ability. The downstream blurring of one hard metric did not produce holism; it produced a vacuum that softer, more privilege-correlated proxies rushed to fill.
The second structural change came from upstream, and it is still accelerating. A medRxiv study examining AMCAS essays from the 2021 and 2024 application cycles found that approximately 12.3 percent of essays in the recent cycle showed high likelihood of AI generation, compared to 2.7 percent in the pre-ChatGPT baseline, with secondary essays (the shorter, school-specific responses that applicants write dozens of times) showing even lower “humanness” scores than personal statements, which suggests that the essay type most susceptible to AI assistance is precisely the one that applicants produce in the highest volume under the tightest time pressure. The practical consequence is that polished writing, which admissions committees have historically treated as a proxy for reflection, communication skill, and authentic self-knowledge, is now available to anyone with a $20 per month subscription, and the signal value of a well-constructed secondary essay has collapsed in the same way that the signal value of a well-designed resume collapsed when word processors replaced typewriters, except this time the compression happened in eighteen months rather than eighteen years. When committees can no longer trust that the voice on the page belongs to the applicant, they do not simply accept the ambiguity; they compensate by weighting other factors they believe are harder to fabricate, which in practice means the MCAT (a supervised, proctored, in-person exam that AI cannot take for you), research conducted under a named principal investigator who will vouch for your contribution, clinical hours logged at institutions that track attendance, and service commitments verified by organizational letterhead.
The MCAT data reveals how narrow the selection band already is and why small shifts in proxy-weighting matter enormously. The average score for all MCAT examinees is approximately 501, while the average for applicants who actually submit to medical schools is 506, and the average for those who matriculate is 512, which means that the admissions process is not selecting from the general pool of people interested in medicine but from a thin, already-elite slice that scored roughly a standard deviation above the test-taking average, a population in which a two-point MCAT difference can move an applicant from the 60th percentile to the 70th and where the difference between acceptance and rejection compresses into a range so tight that the proxies surrounding the score, the school name on the transcript, the prestige of the research lab, the legibility of the service narrative, become the actual decision variables even as committees describe themselves as looking at “the whole person.” Meanwhile, 57.2 percent of applicants and 55 percent of matriculants in the 2025 cycle were women, continuing a six-year streak in which women have been the majority of the medical school pipeline, and the average age at matriculation has crept upward as gap years became the norm rather than the exception, with nearly 60 percent of entering students reporting at least one year between college graduation and medical school enrollment, structural shifts that have diversified the applicant pool along some dimensions even as the credentialing proxies used to evaluate that pool have grown more uniform. The system that emerged from the collision of Step 1 going pass/fail and AI making essays cheaper is not the holistic paradise that admissions brochures describe; it is a system that has lost two of its old signals, one hard and one soft, and replaced them with a constellation of proxies that favor applicants who attended well-known undergraduate institutions, who had access to research opportunities early enough to accumulate publications by age 22, who could afford the time and resources to complete meaningful service that comes with verifiable institutional backing, and who scored high enough on the MCAT to clear a threshold that keeps rising precisely because it is one of the last metrics committees feel they can trust, a system, in other words, that is more proxy-driven at exactly the moment everyone insists it is more holistic, and the only people who benefit from the gap between the rhetoric and the reality are the applicants who already had the most access to the proxies the system now demands.